The State of Dermatology Evidence: Where the Science Is, Where It Isn’t & How AI Is Closing the Gap
SECTION 1
The Dermatology Evidence Landscape: Richer Than Ever, Harder Than Ever to Navigate
Dermatology is in the middle of a therapeutic revolution. 2025 delivered a record number of FDA approvals across inflammatory skin diseases,1 and 2026 has continued the momentum with the approval of icotrokinra (ICOTYDE), the first oral IL-23 receptor antagonist peptide for moderate-to-severe plaque psoriasis.2,3 Hundreds of clinical trials for atopic dermatitis alone are currently active globally,4 and the AAD 2026 Annual Meeting showcased more than a dozen phase 2 and phase 3 trials with practice-changing data across psoriasis, AD, and emerging indications.
Key Milestones Shaping the Current Landscape
| Indication | 2025–2026 Highlights |
|---|---|
| Psoriasis / PsA | Icotrokinra (oral IL-23i) FDA-approved Q1 20262,3; zasocitinib (TYK2i) phase 3 LATITUDE data with biologic-level clearance5; risankizumab vs. deucravacitinib head-to-head (IMMpactful) PASI 90 superiority at week 165; ixekizumab + tirzepatide combination data in PsA with obesity5 |
| Atopic Dermatitis | Hundreds of active trials globally4; rademikibart (anti-IL-4Rα) phase 3 RADIANT-AD sustained at 52 weeks5; lebrikizumab long-term data near-complete clearance to 4 years6; zumilokibart every-3-to-6-month dosing phase 2 data5; amlitelimab (OX40L antagonist, COAST-1 phase 3 results) and other OX40-pathway agents in late-stage development7 |
| Hidradenitis Suppurativa | Povorcitinib (oral JAK1) phase 3 STOP-HS 54-week data: up to 71% HiSCR50, 57% HiSCR75, 29% HiSCR1005; sonelokimab (IL-17A/F nanobody) phase 3 VELA sustained efficacy through week 405; secukinumab approved for pediatric HS8 |
| Emerging Areas | Dupilumab approved for bullous pemphigoid9 and CSU10; delgocitinib first topical JAK inhibitor for chronic hand eczema11; upadacitinib under regulatory review for vitiligo12 |
Although beneficial, this abundance also creates a burden. The AMA's 2025 Organizational Biopsy found 31.5% of dermatologists report symptoms of burnout — and while that figure sits toward the lower end of specialty rankings, the drivers compound with evidence burden in ways unique to dermatology.13 Dermatology carries among the highest note-complexity-per-visit in outpatient medicine.14 The volume and velocity of new evidence are compounding the problem: clinicians and medical affairs teams are expected to track, synthesize, and act on a body of evidence growing faster than any individual or team can manage manually. The challenge is not only volume; it is compounded by an evidence base that is also fragmented across indications, outcome measures, and trial designs, with specific gaps that AI can help surface, map, and close.
SECTION 2
Where the Gaps Are & Why They Persist
Despite the pipeline's richness, critical evidence gaps persist. These gaps create real risk: they slow formulary uptake, leave clinicians making treatment decisions based on indirect comparisons, and give payers reasons to restrict access. Five categories demand attention.
1. Head-to-Head Comparative Data
Active-comparator trials remain the exception in dermatology. A systematic review found significant inconsistencies in design, analysis, and reporting across available head-to-head psoriasis studies.15 In AD, the Heads-Up trial (upadacitinib vs. dupilumab) remains one of very few direct comparisons, and the pipeline's rapid expansion is outpacing the generation of comparative evidence.15,16
2. Real-World Evidence and Long-Term Outcomes
A 2025–2026 Tufts CSDD/Verana Health benchmarking study found that dermatology organizations primarily use RWD for post-marketing safety and burden-of-disease assessments, but underutilize it for comparative effectiveness, treatment sequencing, and outcomes-based contracting.17 Long-term data beyond 2–3 years remain sparse for most newer biologics and JAK inhibitors.
3. Evidence in Underrepresented Populations
Dermatology Times' 2025 Year in Review identified skin health equity as a defining theme, noting higher disease prevalence and worse outcomes among children of color with AD, compounded by limited specialist access.18 Registry analyses document persistent underrepresentation of Black/African American patients across acne, atopic dermatitis, and psoriasis; elderly and pediatric subgroups are also consistently underrepresented.19,20
4. Outcome Measure Consistency
Expert analysis identified 22 key parameters that vary across AD phase 3 trials,21 including comparator design, rescue treatment rules, washout periods, and imputation methods. This variability limits cross-trial comparability and the reliability of network meta-analyses.
5. Site-Specific and PRO Evidence
A systematic review of 454 RCTs using the DLQI found psoriasis dominated PRO-focused research (55.3%), while AD (5.7%), urticaria, and HS remained far less represented.22
Evidence Gap Heat Map: Indication × Evidence Type*
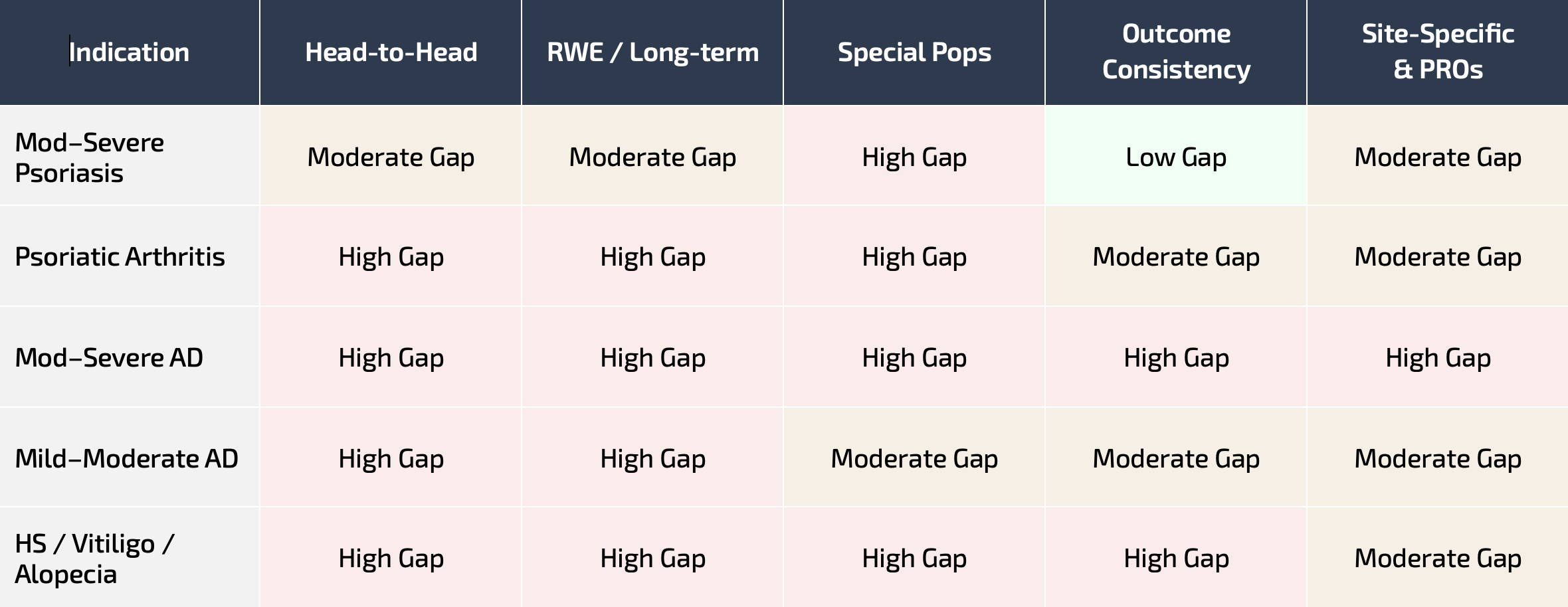
High Gap = critical unmet need; little to no reliable evidence | Moderate Gap = some evidence exists, meaningful gaps remain | Low Gap = well-addressed; evidence is robust and decision-ready
*Gap ratings reflect Atheris Group analysis of published evidence across head-to-head trials, real-world evidence, clinical trial diversity, outcome measure consistency, and PRO research (refs. 15–36).
The Strategic Reality
There is more evidence than ever, more gaps than teams can track, and the distance between what stakeholders expect and what most organizations can deliver continues to grow. The question for medical affairs leaders is how to adopt AI to close this gap, not whether to.
SECTION 3
How AI Is Closing the Gap for Dermatology Professionals & Medical Affairs Teams
AI has moved from research promise to clinical reality in dermatology. A comprehensive review identified fifteen regulatory-approved AI devices in dermatology globally, including three FDA-approved systems in the US, with applications spanning skin cancer detection, screening, and diagnostic support.37 A 2026 review in the Journal of Investigative Dermatology described how generative AI and machine learning are advancing precision medicine for inflammatory skin diseases through deep phenotyping, disease characterization, drug discovery, and clinical care delivery.38
The highest-value applications extend beyond diagnostics, into the workflows where dermatology professionals lose the most time and make the highest-stakes decisions: study design, protocol development, evidence synthesis, and patient management.
For Clinical Researchers: Smarter Study Design and Protocol Development
Clinical trial failure in dermatology remains a significant challenge.39
60% of clinical trials require protocol amendments, half of which are avoidable. Each day a trial extends past its enrollment deadline costs $600K–$8M in lost market opportunity.39
AI is changing this at the design stage:
Protocol optimization: The ClinicalReTrial framework (2026 Preprint) demonstrated that multi-agent AI systems could improve 83.3% of analyzed clinical trial protocols, increasing predicted success probability by 5.7%.40
Industry adoption: Bristol-Myers Squibb announced partnerships with Faro Health and Evinova to transform protocol design through AI. The EMA and FDA jointly issued ten guiding principles for responsible AI use in drug development.41
Dermatology-specific applications: Large language models can produce viable dermatology trial proposals (JMIR Dermatology, 2026).42 AI-powered imaging platforms now provide automated severity grading that reduces inter-rater variability and accelerates patient screening.43
For Practicing Dermatology Professionals: Better Decisions, Less Burden
With icotrokinra, zasocitinib, deucravacitinib, and multiple biologics now competing across overlapping indications, treatment selection has become a complex, multi-variable decision. AI can help in two critical ways:
Clinical decision support: AI systems trained on dermatology-specific data can integrate patient phenotypes, treatment history, comorbidities, and the latest comparative evidence to surface decision-relevant information. The role is to augment clinical judgment with a completeness no individual can replicate manually.38
Administrative relief: A JAMA Network Open study of 263 clinicians found that ambient AI scribe deployment reduced burnout from 51.9% to 38.8% in just 30 days, with significant improvements in after-hours documentation time.44
52 → 39% Burnout rate among clinicians after 30 days of ambient AI scribe deployment (263 clinicians; JAMA Network Open, 2025).44
For Medical Affairs Teams: Proactive, Intelligence-Driven Evidence Strategy
The MAPS 2025 guidance on Strategic Integrated Evidence Generation Planning establishes the framework medical affairs teams are now expected to operate against.45 AI expands what is possible across priorities, particularly adaptive planning, stakeholder-aligned evidence, and gap prioritization:
Continuous landscape monitoring: AI can scan publications, congress data, regulatory filings, and social listening feeds in real time, replacing quarterly manual reviews that are often outdated by the time they are completed.46
Automated gap identification: Map your product's evidence profile against stakeholder decision frameworks (payer, prescriber, guideline body) to identify exactly where investment will yield the greatest return.17,46
Evidence generation strategy at scale: AstraZeneca Spain's evidence generation framework demonstrates how AI analytics and visualization tools are transforming evidence communication to stakeholders.46 AI-enabled protocol design, predictive site selection, and digital endpoints are now considered foundational to modern clinical trial execution.47
The AI-Augmented Dermatology Workflow: Before and After
| Workflow | Without AI | With AI |
|---|---|---|
| Protocol Review & Gap Analysis | Weeks of manual cross-referencing against prior trials and current guidelines | AI-assisted review surfaces design risks, comparator gaps, and endpoint issues in hours |
| Evidence Landscape Scan | Quarterly manual reviews; often outdated by completion | Continuous automated monitoring with real-time competitive alerts |
| Patient Severity Scoring | Subjective clinician scoring with inter-rater variability | AI imaging delivers standardized, reproducible severity grading |
| Treatment Sequencing | Individual knowledge + fragmented guidelines across multiple agents | AI synthesizes patient data, RWE, and guidelines into personalized recommendations |
| Trial Enrollment Optimization | Broad criteria, slow recruitment, frequent mid-trial amendments | Predictive modeling identifies optimal criteria and high-yield sites upfront |
Each of the tools and studies above addresses one slice of the problem. What dermatology professionals and medical affairs teams need is an integrated approach built specifically for the indications, outcome measures, and decisions that define this field.
SECTION 4
The Atheris Approach: IMPACTDermatology
Dermatology-specific AI is not a general-purpose model with a derm prompt layer. It requires domain architecture that horizontal tools cannot replicate.
Dermatology has its own evidence architecture, its own outcome measures (EASI, PASI, IGA, DLQI, SCORAD, IHS4), its own trial design conventions, and its own stakeholder dynamics. Atheris calls this a dermatology brain: domain-specific intelligence that understands the nuances of inflammatory skin disease evidence, the regulatory landscape for biologics and small molecules, and the real-world complexities of clinical practice.
Classification Architecture: What Dermatology-Specific AI Requires
Four requirements distinguish AI built for dermatology from horizontal tools with a derm prompt layer. These are the principles Atheris is built around.
| Requirement | What It Means | Why Generic AI Falls Short |
|---|---|---|
| 1. Curated, Validated Evidence Corpus | Indication-specific literature, trial registries, regulatory documents, congress data for each drug | General-purpose LLMs lack governance over source currency; without a curated corpus they conflate indications and fabricate trial details |
| 2. Outcome Measure Fluency | Native understanding of EASI, PASI, IGA, SCORAD, DLQI, IHS4, vIGA-AD, HECSI, IGA-CHE, with documented limitations of each | Generic models lack structured representation of outcome measures and their psychometric properties; specialty work requires this as an explicit layer |
| 3. KOL-Validated Logic | Proposed validator network to be managed through tracked outreach workflow with conflict-of-interest gates and structured Delphi exercises | Benchmarking against generic medical Q&A misses specialty-specific reasoning errors |
| 4. Indication-First Architecture | Models built around disease (not drug class) reflecting how clinicians and payers think. Deduplicates findings against stable finding keys | Drug-class framing breaks down at lifecycle expansion and combination therapy; LLMs inflate risk counts by surfacing the same issue multiple times |
IMPACTDermatology Illustrative Use Cases in Practice
The requirements above are not theoretical. IMPACTDermatology applies a curated dermatology evidence corpus, structured outcome-measure fluency, KOL-validated reasoning, and indication-first architecture to the highest-stakes workflows in dermatology medical affairs and clinical development.
Application A: AI-Assisted Protocol Review for a Phase 3 AD Trial
IMPACTDermatology reviews a Phase 3 AD protocol by benchmarking its design choices against the indication-specific evidence base: every approved and late-stage AD trial, with their endpoints, comparators, rescue rules, washout periods, and amendment histories tracked at the parameter level. The system flags where the draft diverges from validated precedent, including an EASI threshold tighter than the 22-parameter consensus range, a rescue-medication rule that prior trials amended mid-study, an absent vIGA-AD endpoint where regulators have come to expect one, and outputs a structured review for the sponsor team to evaluate. ImpactDerm extracts indication-specific design intelligence and surfaces issues. Clinical experts make design calls.
Application B: Investigator Network Intelligence for a Phase 3 AD Program
IMPACTDermatology ranks candidate investigators by scoring the available pool across five dimensions: KOL tier (publication record, guideline involvement, prior PI history), site capacity (active trial load, historical enrollment performance), indication fit (depth of prior AD/atopic-disease trial work), geography (regional access to target enrollment populations, including skin-of-color catchment per FDA Diversity Action Plan expectations), and phase history (prior phase 3 experience and amendment rate). The system outputs a tiered investigator list with rationale per dimension and explicitly surfaces gaps in geographic coverage and capacity constraints that sponsor-internal lists routinely miss.
Closing the evidence gaps described above will require infrastructure that combines indication-specific knowledge, validated reasoning, and the kind of layered classification architecture detailed in Section 4. Atheris Group develops dermatology-specific solutions, like IMPACTDermatology, built against these requirements. Let's explore what AI-supported dermatology strategy looks like for your team.
References
Dermatology Times. "Transformative Advances This Year and Beyond." December 29, 2025.
HCPLive. "Q1 2026 Recap: Dermatology News and Updates." April 2026.
Johnson & Johnson. FDA Approval of ICOTYDE (icotrokinra). Press Release. March 18, 2026.
ClinicalTrials.gov. Active interventional studies, condition: atopic dermatitis. U.S. National Library of Medicine. Accessed May 2026.
HCPLive. "ABCs in Dermatology: Late Breaking Data Spotlight at AAD 2026." April 2026.
Weidinger S, et al. "Efficacy and Safety of Lebrikizumab is Maintained up to 4 Years…" AAD Annual Meeting, March 2026. NCT05916365.
Amlitelimab COAST 1 phase 3 study results. Sanofi. September 4, 2025. (NCT06130566.)
Novartis. Cosentyx receives FDA approval for pediatric patients aged 12+ with moderate to severe hidradenitis suppurativa. Press Release. March 13, 2026.
Sanofi/Regeneron. Dupixent approved in the US as the only targeted medicine to treat patients with bullous pemphigoid. Press Release. June 20, 2025.
Regeneron Pharmaceuticals. Dupixent approved in the US as the first new targeted therapy in over a decade for chronic spontaneous urticaria. Press Release. April 18, 2025.
LEO Pharma. Anzupgo (delgocitinib) cream is now the first and only FDA-approved treatment for moderate-to-severe chronic hand eczema in adults. Press Release. July 23, 2025.
Passeron T, et al. Efficacy and safety of upadacitinib in vitiligo: Viti-Up. AAD Annual Meeting, March 2026. (NCT06118411.)
AMA Organizational Biopsy Survey. Medical Economics. May 2026.
PatientNotes / athenahealth. "Physician Burnout & Documentation Burden 2026." March 2026.
Wan MT et al. Head-to-head trials of systemic psoriasis therapies: a systematic review. J Eur Acad Dermatol Venereol. 2019;33(1):42-55.
Silverberg JI, Guttman-Yassky E, et al. Lancet. 2025. doi:10.1016/S0140-6736(25)01865-3.
Tufts CSDD / Verana Health. "The Use of Real-World Data and Evidence in Clinical Trials." Applied Clinical Trials. April 2026.
Dermatology Times. "2025 Year in Review: Strides for Skin Health Equity." April 2026.
Mineroff J, Nguyen JK, Jagdeo J. Racial and ethnic underrepresentation in dermatology clinical trials. J Am Acad Dermatol. 2023;89(2):293-300.
Sevagamoorthy A, et al. Racial and ethnic diversity of US participants in dermatology clinical trials. J Dermatolog Treat. 2022;33(8):3086-3097.
Bao L et al. Expert Perspectives on Key Parameters that Impact Interpretation of RCTs in Moderate-to-Severe AD. Dermatol Ther (Heidelb). 2022;12(2):379-395.
Vyas J et al. Systematic review of 454 RCTs using the DLQI. Br J Dermatol. 2024;190(3):315-333.
Garg A, Cohn E, Midgette B, Frasier K, Strunk A. Efficacy and safety of medical interventions for moderate to severe hidradenitis suppurativa: a living systematic review and network meta-analysis. JAMA Dermatol. 2025. doi:10.1001/jamadermatol.2025.1976
Pham C, et al. Efficacy of biologics for hidradenitis suppurativa: a network meta-analysis and meta-regression for baseline disease severity. Australas J Dermatol. 2025. doi:10.1111/ajd.70085
Mohammed AA, Lengyel AS, Meznerics FA, et al. Efficacy and safety of JAK inhibitors in the management of vitiligo: a systematic review and meta-analysis. Dermatol Ther (Heidelb). 2025. doi:10.1007/s13555-025-01397-z
Babul A, Mehta D, Soliman Y, Hussain M, Babul N. Comparative efficacy of JAK inhibitors indicated for severe alopecia areata: a Bayesian network meta-analysis and matching-adjusted indirect comparison. J Dermatol. 2025. doi:10.1111/1346-8138.17959
Aceituno D, Fawsitt CG, Power GM, et al. Systematic review and indirect treatment comparisons of ritlecitinib against baricitinib in alopecia areata. J Eur Acad Dermatol Venereol. 2025;39(6):1134–1142. doi:10.1111/jdv.20372
Kimball AB, Kirby J, Ingram JR, et al. Burden of hidradenitis suppurativa: a systematic literature review of patient reported outcomes. Dermatol Ther (Heidelb). 2024;14:83–98. doi:10.1007/s13555-023-01085-w
Rosmarin D, Passeron T, Pandya AG, et al. Two-year topical ruxolitinib treatment for nonsegmental vitiligo (TRuE-V3): a randomized, double-blind, vehicle-controlled study. N Engl J Med. 2023;389:1445–1455. doi:10.1056/NEJMoa2310032
Piraccini BM, Cedirian S, Pampaloni F, et al. Effectiveness and safety of baricitinib in severe alopecia areata: 48-week results from a multicenter real-world study. J Eur Acad Dermatol Venereol. 2026;40(2):224–231. doi:10.1111/jdv.70067
Roque JA Jr, et al. Disparities in hidradenitis suppurativa clinical trials: an updated review of ClinicalTrials.gov from 2020 to 2024. J Drugs Dermatol. 2025;24. doi:10.36849/JDD.9066
Holla S, Mora Hurtado AC, Gonzalez S, et al. Racial and ethnic diversity in vitiligo clinical trials: a retrospective cross-sectional study assessing demographic reporting of participants. J Drugs Dermatol. 2024;23(7):e164–e166. doi:10.36849/JDD.8117
Elsanadi R, Esse I, Phong C, et al. Alopecia areata clinical trial enrollment and retention outcome factors among underrepresented ethnic and racial groups: a cross-sectional study. J Am Acad Dermatol. 2023;89(6):1253–1256. doi:10.1016/j.jaad.2023.07.003
Xia E, Li SJ, Drake L, et al. An assessment of current clinician-reported and patient-reported outcome measures for alopecia areata: a scoping review. J Invest Dermatol. 2023;143(7):1133–1142. doi:10.1016/j.jid.2023.02.015
Duponselle J, Herbelet S, Delbaere L, et al. A quality analysis of the measurement properties of clinician-reported outcome measures for vitiligo: a systematic review. J Clin Med. 2025;14(8):2548. doi:10.3390/jcm14082548
Darchini-Maragheh E, Moussa A, Yoong N, Bokhari L, Jones L, Sinclair R. Alopecia areata-specific patient-reported outcome measures: a systematic review. JAMA Dermatol. 2025;161(4):421–429. doi:10.1001/jamadermatol.2024.6660
Nahm WJ et al. AI in Dermatology: Comprehensive Review of Approved Applications. Int J Dermatol. 2025;64(9):1568-1583.
Tang AS et al. AI-enabled precision medicine for inflammatory skin diseases. J Invest Dermatol. 2026 (in press). doi:10.1016/j.jid.2025.10.596.
Getz KA, et al. New Benchmarks Characterizing Protocol Amendment Practices. Tufts CSDD; Applied Clinical Trials. 2024.
Xing S et al. ClinicalReTrial: Clinical Trial Redesign with Self-Evolving Agents. arXiv:2601.00290. January 2026.
Guiding Principles of Good AI Practice in Drug Development. FDA & EMA. January 14, 2026.
Hauptman M et al. Leveraging AI LLMs for Writing Clinical Trial Proposals in Dermatology. JMIR Dermatol. 2026;9:e76674.
QuantifiCare / Legit.Health. First AI-Powered Dermatology Imaging Platform for Clinical Trials. Press Release. August 2025.
Olson KD et al. Use of Ambient AI Scribes to Reduce Administrative Burden and Professional Burnout. JAMA Network Open. 2025;e2534976.
Medical Affairs Professional Society (MAPS). Strategic Integrated Evidence Generation Planning: Guidance. February 2025.
Medina J et al. Shaping the Future of Evidence Generation: RWD to Drive Healthcare Transformation. Pharm Med. 2026;40(2):95-106.
Clinical Leader. CRO Industry Outlook 2026: The Next Stage of Clinical Trial Transformation. 2026.